
The thin line arrives at Washington
The thin line between normality and catastrophe: Part 3


{kind=link}
This is article 7 in the Psyverse #2 series (and article 3 in the Thin line series). For previous articles, see the compendium.
This piece will draw heavily from an excellent article, A Different Approach: The crash of TWA flight 514 by Admiral Cloudberg, and Chapter 7 of Delivering the Right Stuff by Andrew J. Dingee. I recommend reading both for more information.
On the 1st of December 1974, a plane crashed into a mountain. It was not the first one in history to do so, nor the last. In isolation, the crash of Trans World Airlines (TWA) flight 514, tragically killing all 92 people on board, holds no more significance than any other deadly plane crash. Why flight 514 is considered one of the most influential accidents in aviation safety history has little to do with the crash itself, but with a near miss six weeks earlier.
In October 1974,1 a plane nearly crashed into a mountain. 40 miles out, at an altitude of 7,000 feet, flight controllers cleared a United Airlines flight for an instrument approach to Washington Dulles Airport without a minimum altitude.2
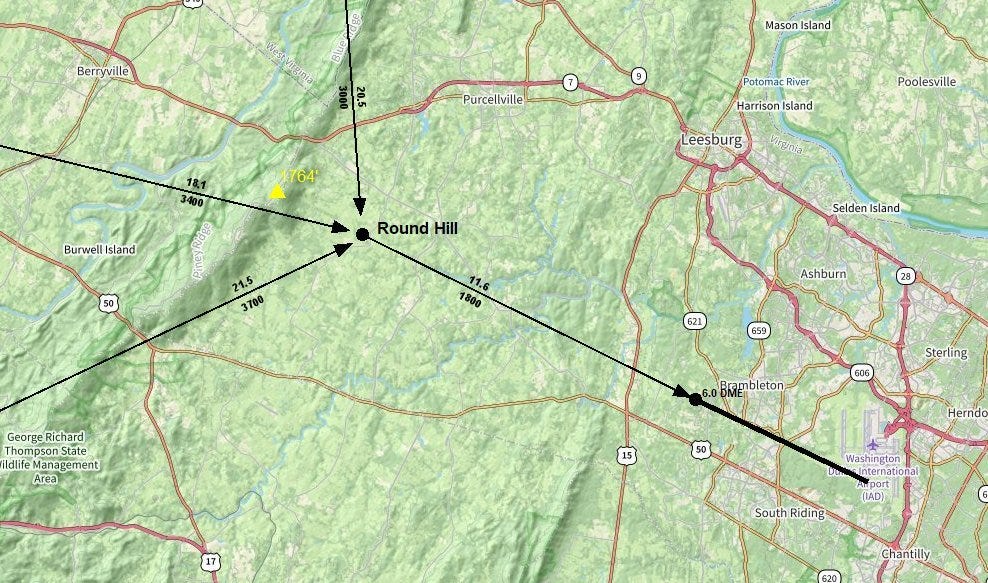
On the plan view of the Dulles “approach plate” (see Fig 1 below) three official flight paths - each with associated distance (indicated above path) and minimum altitude (below path) - converged to the Round Hill beacon point, or “initial approach fix”, 11 nautical miles (NM) out from the “final approach fix”. From Round Hill, a single flight path led to this “final approach fix” 6 NM out from Runway 12.3
On the profile view of the approach plate, on the other hand, only the final approach fix and the final 6 NM are displayed with a minimum altitude of 1800 feet. The flight path from Round Hill, with accompanying minimum altitude,4 to the final approach fix is not displayed. This discrepancy is what likely led to the United Airlines flight near miss.
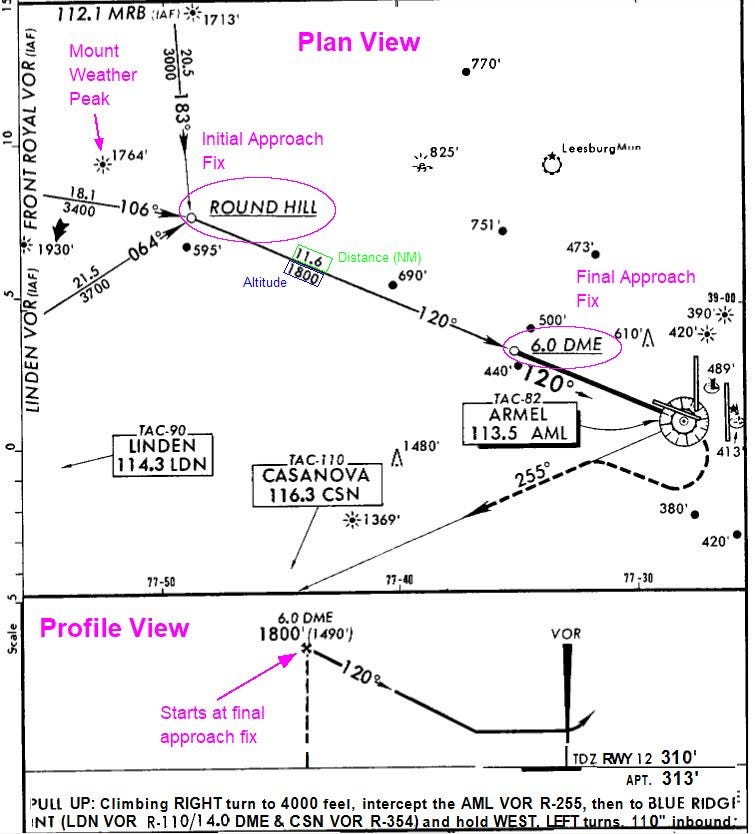
When Air Traffic Control (ATC) cleared the United Airlines flight for an approach to land without a minimum altitude clearance, the pilot assumed they could descend to the minimum altitude of 1800 ft, clearly displayed on the profile view approach plate.5
Fortunately for the United Crew, they were in good weather conditions and could see that they were about to fly dangerously close to the peak of Mount Weather, so they adjusted accordingly.6 After landing, the pilots filled out an incident report and sent it to the United Airlines Event Review Committee (ERC). This was part of a new procedure as part of a program put in place by United in January 1974 called the Flight Safety Awareness Program. Once the report was reviewed by the ERC, a safety alert was sent out to all United Pilots about the Dulles Runway 12 approach discrepancy. But only United Pilots. Pilots employed by other airlines never saw this incident report – no federal system was in place to facilitate distribution.
The crash of Flight 514
One hour before Flight 514 crashed into a mountain, the pilots of an American Airlines flight made the same mistake that United’s pilots had made six weeks earlier. Seven miles out from Mount Weather, at 1800 ft, the American Airlines plane was heading straight towards the mountain. This time, the weather conditions were poor. The pilot decided to radio ATC at Dulles to ask what altitude they should be at. ATC told them to climb to 3,400 feet immediately. A crash was averted, for an hour.7
TWA Flight 514 took off from Port Columbus International Airport8 at 10:24 am, heading for Washington National Airport. But twelve minutes after take-off, the pilots were ordered to divert to Dulles airport - severe weather (high winds, snow and rain) had resulted in the closure of Washington National.9
Due to the diversion, the plane did not initially follow the official published flight path - instead intercepting the 300 degree (120 degree on the approach plate) radial 13km earlier than the plate’s initial approach fix at Round Hill.

At 11:04, 44 NM from Dulles Airport, ATC cleared flight 514 to approach runway 12, again without a minimum altitude. Just like the United and American Airlines flights, the pilot descended to 1800 ft, thinking the ATC had implicitly given him clearance and would point out if he was at the wrong altitude.10
While they were descending, the pilot had another look at the approach plate and noticed that “this dumb sheet says it’s thirty-four hundred [feet] to Round Hill — is our minimum altitude”. Due to confirmation bias, a discussion on this discrepancy was cut short before it could even begin.11 All the crew managed to miss the Mount Weather peak heights of 1764 and 1930 feet, which they were directly flying over.12
Once they reached 1,800 feet, they encountered significant turbulence and downdrafts, causing frequent altitude oscillations. They received only two altitude warnings: the first, seven seconds before impact, and the second, two seconds before impact. It was too late for the pilots to take any corrective action, and the plane crashed into Mount Weather, killing everyone on board.13
After the NTSB released their report of the Flight 514 crash, the FAA sprang into action and introduced what would become the Aviation Safety Reporting System or ASRS. The story of Flight 514 is often told as the turning point in the development of the ASRS, with the unique set of circumstances surrounding the crash being the key motivator. It is therefore interesting to note the nearly identical crash that occurred six years earlier.
Groundhog day
On the 25th of October 1968, a plane crashed into a mountain. It was not the first one in history to do so, nor the last. In isolation, the crash of Northeast Airlines Flight 946, tragically killing 32 out of 42 occupants, holds no more significance than any other deadly plane crash. Out of isolation, this remains the case. Why flight 946 is considered just another accident in aviation safety history, has little to do with the crash itself (or the previous near miss), but the continuing inaction of the FAA.
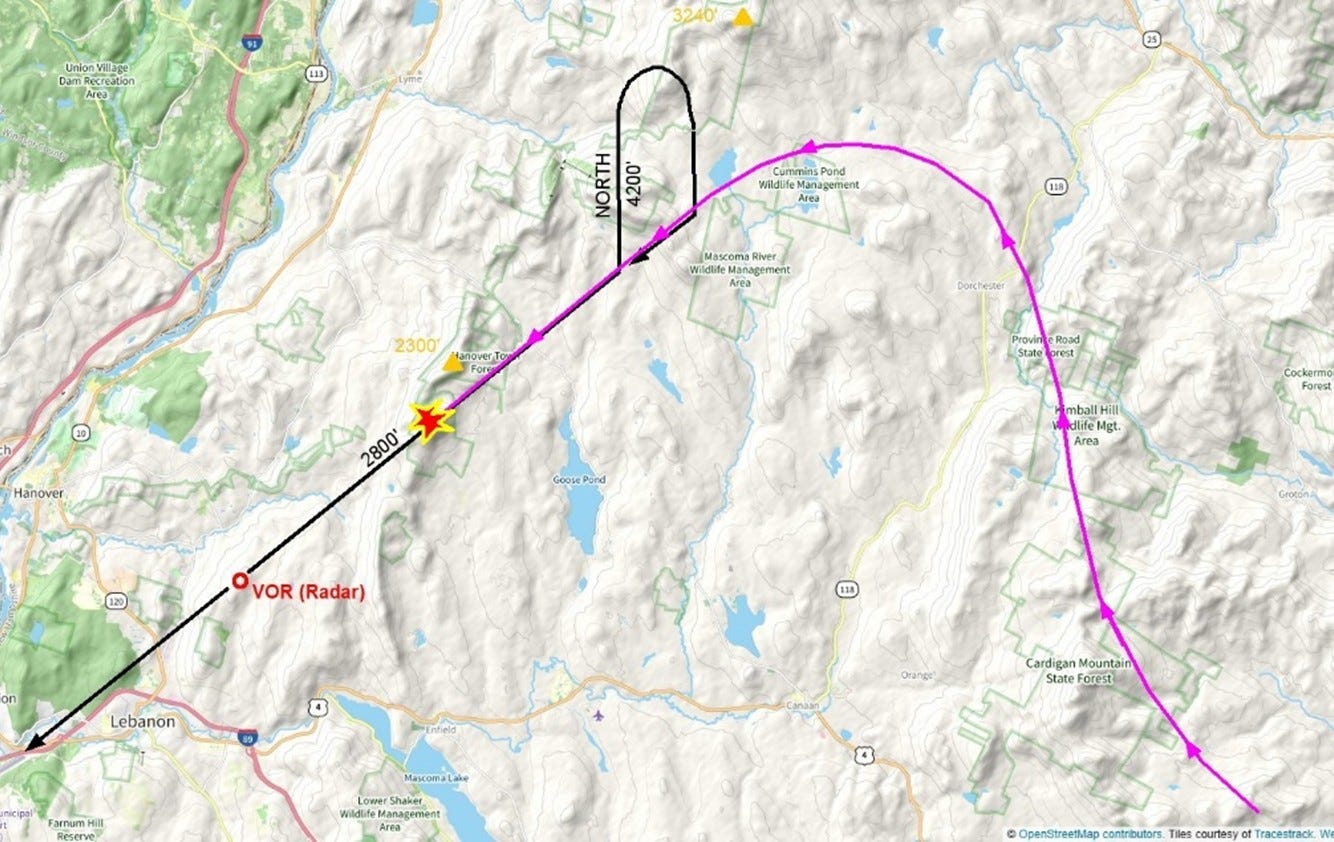
The runway 25 approach plate of Lebanon Municipal Airport, North Hampshire, from 1968 looks confusing, to say the least. Since only one radar station existed without distance measuring equipment (i.e. just VOR, no DME),14 and the airport was nestled in amongst a very hilly region, the entirety of the approach plate flight paths were restricted to one single radial.

A flight at cruising altitude coming in from any direction was supposed to first head to the VOR (radar) station location, then head northeast (radial 066 degrees) for around 10 Nautical Miles. During this phase, flights could not descend below 4200 ft. This point – 10 NM from the VOR – can be thought of as the start of the final approach (see Fig 6, indicated by purple circle), but is not an official “fix”.
Flying north, a pilot was supposed to circle around in a clockwise direction – ensuring a minimum altitude of 4200 feet throughout - eventually ending up inbounds, travelling towards the VOR radar station and Lebanon runway 25 (the 246 degree radial). The flight was then supposed to descend to a minimum altitude of 2800 feet. Only once the pilot had passed the VOR station, could they descend no lower than 1800 feet until they could fly under Visual Flight Rules or “the time to fly to the airport had been flown”.15

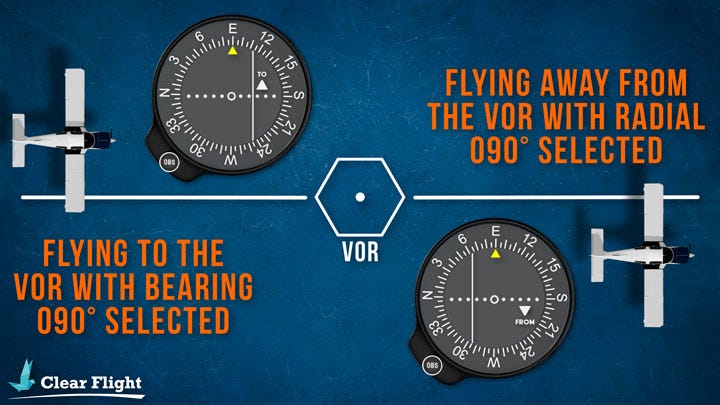
The problem with this approach centres on the radar system. A VOR station can only provide a pilot with information about which radial it is on in relation to the station, and whether flying along that radial would take you towards (TO) or away from (FROM) the radar station. So, when coming into land at runway 25, the indicator on a pilot’s Course Deviation Indicator (CDI) would have a radial of 246 degrees selected, with “TO” on the display. As the plane passed over the VOR radar station, this “TO” would switch to “FROM”. There is a nice explanation on how this works from Clearflight.
At some point before Flight 946 crashed, a Northeast Airlines flight was coming in to land at runway 25. It was overcast, with occasional breaks in cloud. The pilots saw the needle on their display jump and the CDI switch from “TO” to “FROM”. Thinking they had just passed the VOR station, they started to descend. Once they reached 2000 feet, the pilots noticed the CDI had switched back to “TO”. The captain then saw how close they were to the ground through one of the breaks in the cloud and immediately climbed back up to a safe altitude.
Once they had safely landed, they reported this incident to the local FAA maintenance technician, who checked the VOR radar station and found no irregularities. The pilot “did not, nor was he required to by [the FAA’s] current procedures … [to] report this occurrence to any central unit within [the FAA].”16
Flight 946 took off 47 minutes late from Boston. It was late in the evening, sunlight was fading, and the conditions were overcast with occasional breaks in cloud. Arriving into the vicinity of Lebanon, the crew communicated to ATC that they were going to perform a “standard instrument approach”. For some reason, the crew decided not to perform the published instrument approach procedure.17
Flying due north-west, flight 946 attempted to take a shortcut, avoiding the initial VOR station approach starting point entirely. They tried to tack on to the very end of the approach procedure, turning anticlockwise onto the final approach path.
The flight then continuously descended, not stopping at the minimum altitude of 2800 feet, until they eventually crashed into the top of a rocky, heavily wooded mountain, 2237 feet above sea level.
In the subsequent investigation, the NTSB tested for possible interference that could affect a pilot’s CDI display. They found areas along the approach where “course roughness manifested itself on the Course Deviation Indicator” but could not recreate the switch from “TO” to “FROM”. The NTSB concluded that the probable cause of the crash was the premature descent based on navigational instrument indications that they were about to pass the VOR station.
Due to the potential for an incident report from the previous near miss preventing the deadly crash of Flight 946, the NTSB believed that “the FAA should provide the leadership in developing and implementing an industrywide operational incident reporting system”. The FAA responded with:
In regard to the suggested industrywide operational incident reporting system, this is now being accomplished by our system of issuing telegraphic alerts and operations bulletins […]. We will conduct a complete review of current incident reporting procedures.18
On the 1st of December 1974, TWA Flight 514 crashed into a mountain. So the FAA quickly introduced an actual industrywide operational incident reporting system, at least six years too late.
The series within a series continues next week.
If you enjoyed today’s article, please consider gifting a heart ❤️, restacking 🔄 or sharing 🔗. It would be much appreciated.
If you enjoyed today’s article, please consider gifting a heart ❤️, restacking 🔄 or sharing 🔗. It would be much appreciated.
If you enjoyed today’s article, please consider gifting a heart ❤️, restacking 🔄 or sharing 🔗. It would be much appreciated.
If you enjoyed today’s article, please consider gifting a heart ❤️, restacking 🔄 or sharing 🔗. It would be much appreciated.
If you enjoyed today’s article, please…

The only detailed info I could find on this particular flight comes from the book “Delivering the Right Stuff”. Which says the near miss occurred in November 1974. However, this book does not have many sources, and the NTSB report on the crash of Flight 514 clearly states that a near miss occurred six weeks earlier. So I am going with the NTSB’s account.
An instrument approach procedure is a set of predetermined manoeuvres that allow an aeroplane operating under Instrument Flight Rules (see part one of the thin line series for explanation on flight rules) to land.
Two different types of radar were available in the 1970s that would provide positional information: Very high frequency Omnidirectional Range station (VOR) and Distance Measuring Equipment (DME). VOR provides a heading (or radial) to the pilot of where the plane is in relation to the station (provides an angle relative to north, but not a distance). DME provides distance information to the pilot of where they are in relation to the station. In combination, these two systems can pinpoint the location of the plane.
I believe Washington Dulles had just installed a VOR/DME system in 1974 (having previously been just VOR). Though I am not sure about this (there is a vague reference to improved radar in Delivering the Right Stuff).
An “approach plate” is the colloquial name for an “instrument approach procedure chart”. Pilots use these plates as a reference when coming in to land for an instrument approach.
The initial approach fix is a reference point to be used by pilots to know when the approach “begins”, when the pilots start the initial segment procedure of the landing. The fix (and other fixes in general) are identified through an intersection of VOR radials, the location of a VOR station itself, a non-directional beacon, or a DME location designation (a distance from a DME station).
The approach plate of Washington Dulles in 1974 has an initial approach fix designated by the Round Hill (I believe non-directional) beacon. The final approach fix (the point at which the final approach starts. The aeroplane is lined up with the runway and is descending to land), was designated as 6 Nautical Miles from the DME on the 120 degree radial (in line with the runway)
Which would likely have started at 3000 ft at the Round Hill beacon.
Pilots were becoming accustomed to ATC’s warning them if they were at too low an altitude.
At this point in aviation history, the introduction of VOR/DME in combination with transponders and computer systems allowed Air Traffic Control (ATC) to fully ascertain a 3D picture of the location and speeds of flights (see here). According to Delivering the Right Stuff, this meant that ATC was becoming more involved in the process of take-off and landing.
Before these technological developments, it was the responsibility of the pilot to communicate altitude and position to the Air Traffic Controller (ATC).
According to a report by Chappell and O’Leary
From Chapter 7 of Delivering the Right Stuff
Renamed to John Glenn Columbus International Airport in 2016
From Northern Viginia Magazine November 2024 article.
According to the NTSB report (which the author originally read in Cloudberg’s article), in the aftermath, FAA witnesses stated that because the flight was not on an official flight path at this point (they crashed before they could reach Round Hill), the responsibility lay with the pilot to ensure altitude and position. The counterposition to this was that Flight 514 was in a radar environment; therefore, the ATC had information on its altitude and position.
The same VFR vs IFR confusion (see part one) reared its ugly head again.
From the NTSB accident report:
The captain said, ‘You know, according to this dumb sheet it says thirty - four hundred to Round Hill is our minimum altitude.’ The flight engineer then asked where the captain saw that and the captain replied, ‘Well, here. Round Hill is eleven and a half DME.’ The first officer said, "Well, but - - - ‘ and the captain replied, ‘When he clears you, that means you can go to your - - - ‘ An unidentified voice said, ‘Initial approach,’ and another unidentified voice said, ‘Yeah!’”
As they were not on an official flight path, in poor weather conditions, they may not have known their precise position until they turned on to the 300 degree radial (120 degree on approach plate)
A couple of extra details:
Six hours after Flight 514 crashed, another plane almost suffered the same fate, due to the same altitude miscommunication between ATC and the pilots.
One of the major developments to come out of the Flight 514 crash was the installation of ground proximity warning systems on all commercial aircraft.
Very high frequency Omnidirectional Range station (VOR) and Distance Measuring Equipment (DME). See Footnote 2 for definitions.
From NTSB report on crash.
The information about the previous near miss comes from the 1969 hearings before the House of Representatives: Aviation Safety and Aircraft Piracy.
While not applicable here, there is a bias called “plan continuation bias”, colloquially known as “Get-there-itis” by pilots, which causes pilots to stick to a flight plan despite warnings from ATC or other indicators showing it would be more dangerous to stick to the plan than change it. In the case of flight 946, the pilots did the opposite, changed the plan without telling ATC.